
VARIANT – 1
Healthcare doesn’t have a denial problem.
It has a predictability problem.
Every day, claims are denied for eligibility mismatches that could have been verified at registration. Prior authorizations are missing. Documentation doesn’t support medical necessity. Modifiers are incorrect. Payer policies changed last month, and no one updated the workflow.
Revenue cycle teams don’t discover these failures when they occur.
They discover them 30-45 days later when cash doesn’t arrive.
These aren’t rare exceptions.
They are structural leaks.
According to reporting from the Healthcare Financial Management Association, average initial denial rates nationally now hover around 10-12%. MGMA benchmarking data continues to show rising denial volumes across physician practices. The American Hospital Association (AHA) has repeatedly highlighted prior authorization and administrative complexity as a growing financial burden for hospitals and health systems.
This is not simply a billing issue.
It is an infrastructure issue.
And the organizations solving it are not building larger appeal teams.
They are redesigning their revenue cycle around AI-driven denial prevention.
The Anatomy of a Claim Denial
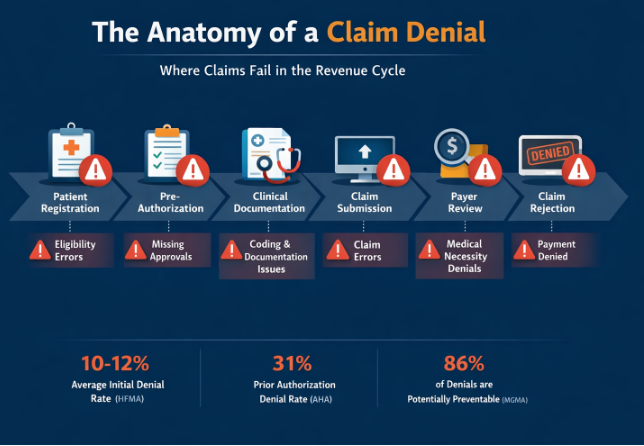
The most important insight this visual reinforces:
Denials do not begin at claim submission.
They originate upstream:
- Patient registration
- Eligibility verification
- Prior authorization
- Clinical documentation
- Coding alignment
- Claim formatting
- Payer review logic
By the time a claim is officially denied, the root cause has already been embedded in the workflow.
That is why reactive denial management will always be more expensive than prevention.
Why Claim Denials Are Increasing
Denials are not increasing randomly. They are increasing structurally.
1️⃣ Payer Policy Complexity Is Accelerating
Commercial payers continuously update:
- Coverage criteria
- Modifier rules
- Documentation thresholds
- Medical necessity definitions
- Authorization requirements
The AHA has documented the administrative burden associated with prior authorization as a growing operational strain. These policy changes are often subtle, payer-specific, and difficult for manual teams to track in real time.
No human team can monitor every rule variation across every payer continuously. AI can.
2️⃣ Administrative Burden Is Already at Capacity
HFMA research consistently identifies administrative friction as one of healthcare’s largest cost drivers.
Revenue cycle teams are already managing:
- Staffing shortages
- Increasing documentation demands
- Escalating appeal volumes
- Payer communication complexity
Adding more manual review does not fix systemic inefficiency.
It compounds it.
3️⃣ Most Denials Are Operational – Not Clinical
A substantial percentage of denials stem from predictable operational errors:
- Eligibility issues
- Missing or expired authorizations
- Documentation insufficiency
- Coding mismatches
- Payer-specific modifier requirements
These are patterns.
And patterns are precisely what machine learning models detect best.
What “Stopping Denials Before They Happen” Actually Means
Stopping claim denials before they happen means identifying denial risk before submission, when correction is still simple, fast, and inexpensive.
It shifts the revenue cycle from:
Reactive → Predictive
Manual review → Intelligent automation
Appeals-based recovery → Structural prevention
This is not about scrubbing claims for missing fields.
It is about predicting whether a payer is likely to reject a claim based on:
- Historical denial behavior
- Payer-specific approval patterns
- Documentation sufficiency
- CPT–ICD alignment
- Authorization compliance
The difference is architectural.
The Denial Prevention Maturity Model
Organizations do not jump directly into AI optimization. They evolve.
Level 1 – Reactive Recovery
- Manual denial work queues
- Appeal-focused
- Limited root-cause tracking
Level 2 – Structured Denial Management
- Categorized denial reporting
- Monthly denial dashboards
- Basic claim scrubbers
Level 3 – Pattern Recognition
- Denial trend analysis
- Root cause correction
- Front-end workflow adjustments
Level 4 – Predictive Prevention
- AI risk scoring pre-submission
- Payer-specific behavior modeling
- Automated authorization intelligence
- NLP-based documentation validation
Level 5 – Autonomous Revenue Intelligence
- Continuous learning models
- Real-time payer rule adaptation
- Proactive denial forecasting
- Near-zero preventable denials
Most organizations today operate between Level 2 and Level 3.
Competitive advantage begins at Level 4.
How AI Stops Claim Denials Before Submission
AI-driven denial prevention operates across five structural layers.
1️⃣ Predictive Claim Risk Scoring
Before transmission, AI models analyze:
- Historical denial outcomes
- Payer-specific approval rates
- CPT–ICD pairing patterns
- Modifier combinations
- Documentation completeness signals
- Authorization alignment
- Patient coverage validation confidence
Each claim receives a denial probability score.
High-risk claims are flagged instantly.
Correction occurs before submission.
Even a 3-4% improvement in first-pass acceptance can translate into millions in protected revenue in mid-to-large systems.
2️⃣ Real-Time Eligibility Intelligence
Many denials originate at registration.
Traditional eligibility checks occur once.
AI continuously revalidates:
- Active coverage
- Coordination of benefits
- Service-level exclusions
- Plan limitations
This eliminates “coverage inactive” denials before service delivery.
3️⃣ Prior Authorization Automation
Prior authorization remains one of the largest denial triggers.
AI platforms:
- Track payer authorization requirements
- Trigger alerts during scheduling
- Monitor approval status
- Escalate delays
- Block submission if authorization is missing
Instead of discovering the problem 45 days later, the issue is resolved before the encounter occurs.
4️⃣ Documentation & Coding Alignment via NLP
Natural Language Processing evaluates clinical documentation in context to ensure:
- Medical necessity elements are present
- Diagnosis codes support procedures
- Required documentation components are captured
- Complexity level aligns with billed service
AI augments coders.
It does not replace them.
5️⃣ Denial Trend Forecasting
Instead of reacting to denial spikes, predictive models identify emerging risk patterns early:
- Sudden drop in approval rate for specific CPT–ICD pair
- New modifier rejection pattern
- Authorization denials rising for specific payer
Prevention becomes proactive, not reactive.
AI vs Traditional Claim Scrubbing
Traditional scrubbers validate formatting.
AI predicts payment probability.
| Capability | Traditional Scrubber | AI Denial Prevention |
|---|---|---|
| Rule Type | Static | Adaptive |
| Payer Awareness | Generic | Payer-specific |
| Documentation Review | Minimal | NLP contextual analysis |
| Risk Scoring | None | Predictive probability |
| Learning Over Time | No | Continuous refinement |
| Intervention Timing | Post-coding | Pre-submission |
The goal is not cleaner claims.
The goal is to pay claims.
The Financial Model Behind Denial Prevention
Executives do not invest in philosophy.
They invest in math.
Consider a health system submitting 120,000 claims annually.
Denial rate: 10%
Average claim value: $1,250
Denied claims annually: 12,000
If 30% are never successfully recovered:
Lost claims: 3,600
Lost revenue: $4.5 million
If AI reduces preventable denials by 35%:
Prevented denials: 4,200
Revenue protected: $5.25 million
This excludes:
- Rework labor savings
- Cash flow acceleration
- Reduced Days in A/R
- Lower appeal overhead
Prevention compounds annually.
Appeal recovery does not.
Is Your Organization Ready for AI Denial Prevention?
Before implementation, assess readiness.
Data Requirements
✔ 18–24 months of structured denial history
✔ Standardized denial codes
✔ Clean payer mapping
✔ Historical authorization records
✔ Documentation availability
Technical Requirements
✔ EHR integration capability
✔ Billing system integration
✔ Secure cloud infrastructure
✔ Real-time data exchange capability
Governance Requirements
✔ Executive oversight
✔ Clear escalation pathways
✔ Defined human-in-the-loop review process
✔ Performance monitoring framework
AI is not plug-and-play magic.
It is operational intelligence layered onto clean infrastructure.
AI Governance & Compliance Considerations
Denial prevention AI must be deployed responsibly.
Key considerations:
- Human oversight remains mandatory
- Recommendations must be auditable
- Models should be explainable
- HIPAA-compliant data handling is essential
- AI must not override a physician’s clinical judgment
High-performing organizations treat AI as decision support, not autonomous adjudication.
Governance maturity differentiates sustainable transformation from short-term experimentation.
Common Executive Misconceptions
“Denials are inevitable.”
Many are predictable and preventable.
“We just need more denial staff.”
More staff increases cost without eliminating structural inefficiency.
“Our scrubber already handles this.”
Scrubbers validate syntax. AI predicts payer behavior.
“We can’t change payer behavior.”
You may not control payer behavior, but you can model and adapt to it.
What ROI Looks Like in Operational Terms
Denial prevention impacts:
- First-pass acceptance rate
- Days in A/R
- Cost to collect
- Net revenue retention
- Appeal labor utilization
Preventing even 2–4% of avoidable denials can materially shift operating margin in high-volume environments.
Unlike appeal recovery, prevention compounds.
Every prevented denial eliminates:
- Rework labor
- Appeal delays
- Write-off risk
- Cash flow volatility
This is structural margin protection.
The Strategic Shift
For years, healthcare organizations normalized 10% denial rates.
They staffed appeal departments.
They built recovery workflows.
They expanded denial management teams.
But denials are not random.
They are signals.
And signals can be modeled.
The competitive advantage in 2026 belongs to organizations that:
- Redesign workflows around predictive intelligence
- Embed AI into front-end revenue cycle
- Treat denials as preventable events, not unavoidable costs
- Move from recovery economics to prevention economics
Final Perspective
Stopping claim denials before they happen is not a billing tactic.
It is a systems decision.
Organizations that remain reactive will continue expanding appeal budgets, hiring more denial specialists, and normalizing 10%+ denial rates as “industry standard.”
Organizations that redesign their infrastructure around predictive intelligence will operate differently.
They will stabilize cash flow.
They will reduce administrative friction.
They will protect margins in tightening reimbursement environments.
They will build operational resilience instead of reactive capacity.
The technology to do this already exists.
The financial case is defensible.
The operational roadmap is clear.
The remaining variable is strategic commitment.
Denials are no longer random events.
They are behavioral patterns driven by payer rules, documentation gaps, authorization complexity, and workflow breakdowns.
And patterns can be predicted.
That is the shift.
The solution is proactive denial prevention using AI that identifies and resolves issues before claims ever leave your organization.
ImpactRCM delivers comprehensive prevention across every stage of the revenue cycle:
- Real-time eligibility verification at scheduling
- Automated authorization management that prevents authorization-related denials
- AI-powered coding validation that eliminates alignment errors
- Pre-submission claim scrubbing that intercepts payer rejection triggers
- Predictive denial analytics that forecast which claims carry elevated risk
- Continuous learning models that improve prevention accuracy over time
The result is structural improvement not temporary recovery gains.
Organizations leveraging this approach reduce denial rates by 25–35%, improve clean claim rates to 95%+, and reallocate staff away from rework and toward higher-value strategic initiatives.
This is not about building a stronger appeals department.
It is about reducing the need for one.
If denial prevention is becoming a strategic priority within your organization, a structured assessment can identify where predictable leakage is occurring and where AI-driven intervention will deliver the highest impact.
Every month of delay compounds preventable revenue loss.
The shift from reactive recovery to predictive prevention is not incremental optimization.
It is structural margin protection.
And it is quickly becoming the standard for high-performing revenue cycle organizations.
FAQ: Predictive RCM & AI
Claim denials are increasing due to:
- Rapid payer policy changes
- Rising prior authorization complexity
- Administrative staffing shortages
- Documentation requirements
- Payer-specific rule variation
The growth in complexity exceeds manual monitoring capacity which is why predictive automation is becoming necessary.
AI prevents claim denials by analyzing historical denial patterns, payer-specific rules, documentation completeness, CPT–ICD alignment, and authorization status before submission. Predictive models assign a risk score to each claim, allowing revenue cycle teams to correct issues before they trigger payer rejection.
The most common causes include:
- Eligibility verification errors
- Missing or expired prior authorizations
- Insufficient documentation for medical necessity
- Coding mismatches between CPT and ICD-10
- Incorrect modifier usage
- Payer-specific policy changes
Many of these are operational and predictable, making them ideal targets for AI-driven prevention.
Organizations implementing AI-driven denial prevention commonly report:
- 25–35% reduction in preventable denials
- 95%+ clean claim rates
- 2–4% improvement in first-pass acceptance
- Reduced days in A/R
Actual results depend on data quality, payer mix, and workflow maturity.
Yes, when implemented properly. AI denial prevention platforms must:
- Maintain HIPAA-compliant data handling
- Provide audit trails
- Offer explainable recommendations
- Include human oversight
- Avoid overriding clinical judgment
High-performing organizations deploy AI as decision support, not autonomous adjudication.